Massage with the Eyes in Your Fingers
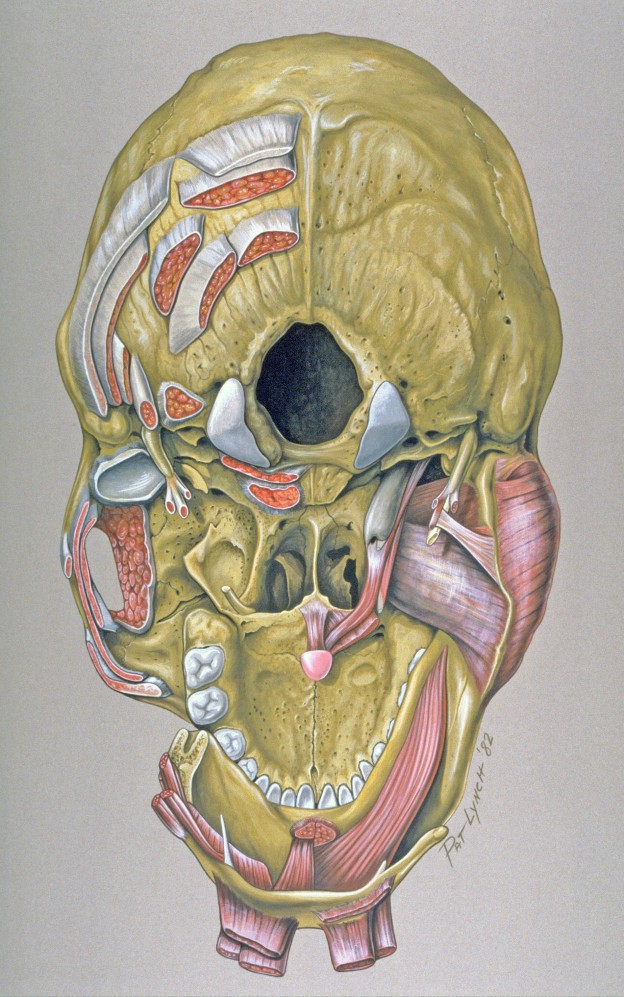
There is a time in every massage when the therapist begins to rub the posterior neck. For many of our computer-burdened clients, it presents an opportunity to relieve the congestion of technology. The head is supported by these many muscles, embedded with many layers, often adhesed, and near the source of many functions from sleep … Continue reading Massage with the Eyes in Your Fingers

